
The razor bumps. The ingrown hairs. The sensitive skin. The tough angles... There are few places on the body more challenging to maintain than the bikini line, as many women have learned struggling to shave, pluck, wax, and laser their way to smooth skin. Even more unfortunate, there are a ton of myths floating around about hair down there. Marisa Garshick, MD, a dermatologist at Manhattan Dermatology & Cosmetic Surgery, reveals the myths she hears patients repeat the most in her office.
Myth: Hair grows back thicker if you shave it
Dr. Garshick says that shaving anywhere on your body will not cause the hair to come back in thicker; diameter will always stay the same over time. “After shaving, the ends of the hairs are simply blunted, as opposed to the natural soft tip, which may cause the hair to seem coarse,” Dr. Garshick explains. “But the actual thickness remains unchanged.” After shaving, she suggests using a mild cleanser and a gentle moisturizer to keep your skin feeling soft and smooth, even when hairs are growing back. Try CeraVe Hydrating Body Wash and Eucerin Original Healing Rich Lotion.
Myth: Tweezing is the best treatment for ingrown hairs
Lots of women think tweezing an ingrown hair is the fastest and most effective way to deal with it, according to Dr. Garshick. They're simply wrong. “Tweezing can lead to trauma of the hair follicle, which will just cause more redness and inflammation,” she explains. “Avoid picking or squeezing as this can lead to scarring.” If you have razor bumps or ingrown hairs, Dr. Garshick says to leave them be. “Often, simply letting the hair grow a little will allow the hair to break free from being trapped in the skin,” she says, at which point you can remove it carefully. You can also use a hot compress to help the point break free. If the ingrown hasn't popped out after a week or two, call your derm, who can extract the ingrown for you.
Myth: You should shave down there every day
A lot of women believe the skin on their bikini line will get used to razoring if they do it daily, says Dr. Garshick, but all that does is bring on more irritation and razor bumps. Wait until a few millimeters of hair are visible, or about two days. To reduce your risk of sensitivity, shavein the direction of the hair growth with a clean razor blade that you replace after five to 10 shaves. “Sometimes a prescription for a topical steroid may be needed to treat razor bumps, but you should discuss this with a specialist,” says Dr. Garshick. “And if you're looking for a more long-term option, laser hair removal can help.”
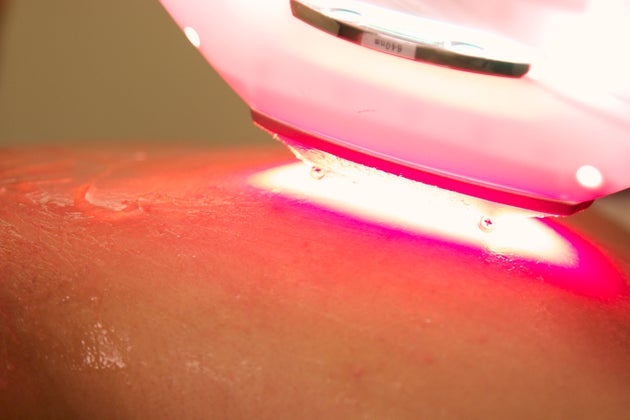
Myth: It's smart to wax between laser hair removal treatments
Laser hair removal treatments from a board-certified dermatologist leave you hair-free in five to eight treatments. The key: five to eight treatments, not one or two. The laser specifically targets growing hairs, which is only a portion of your total hairs, Dr. Gars hick explains. “Although you will notice a significant improvement after your laser hair removal sessions, you may still notice some hairs that don't go away right away,” she says. “Do not attempt to remove this hair with waxing, because the laser targets the pigment in the hair. If the hair has been removed, the laser can't do its job.” Dr. Gars hick says to leave the hair alone. Don’t wax, pluck, or bleach between laser hair treatments, although it’s okay to shave, which will still allow the hair to be zapped by the laser during your next treatment.
It’s totally OK to have body hair, but if you do decide to remove it, you may not be exactly sure which method is best. Laser hair removal and waxing are two popular procedures that women and men can book at a salon or spa. Yet, there are still big misconceptions tied to them — including the rumor that laser treatment doesn’t work on black people, and wax rips your skin off.
To debunk common myths about these two hair removal techniques, we turned to Spruce & Bond specialist Kristen Rogers to set the record straight. Scroll down to find out what we learned about the difference between laser and waxing. Then, share your hair removal stories in the comments section. FERYJORY VIA GETTY IMAGES
It is more about the color of the hair rather than texture or complexion when determining if laser hair removal will work for you.
MYTH: Black people can’t do laser hair removal.
According to Rogers, there is no skin type or tone that laser will not work on. It is more about the color of the hair rather than texture or complexion. “There are different settings and machines for different skin types, which makes it possible for all skin tones to do laser,” she says.
FACT: The darker your body hair is, the better for laser hair removal.
Individuals with dark hair are prime clients for this method. Basically, the more contrast there is between your skin tone and hair color, the better. Rogers doesn’t believe people with blonde, red or gray hair will benefit from laser.
MYTH: You must be close-shaven before getting laser hair removal.
While Rogers says that most of her clients prefer to shave the areas where they will get laser treatment, it isn’t uncommon for the aesthetician to shave an area such as the bikini line. “It is scary and difficult for them,” she explains. “The only downside to having the specialist shave you in the room, is that it is a dry shave.”
FACT: It takes more than one laser hair removal session to see a significant reduction in hair growth.
“Laser hair removal works as a continuous process of removing the hair follicle of the given area over a specific amount of time,” says Rogers. “The laser works under the skin’s surface to damage the hair follicles and stunt future growth.” The professional notes that you should start to see results within two weeks of your first treatment. As the hair grows back slower, it will be very patchy. She adds, “I always recommend my clients to treat at least five times, spaced apart four to six weeks, to see the best results. Each session reduces hair growth by 10 to 15 percent.”
MYTH: You won’t experience any pain during laser hair removal.
It isn’t out of the ordinary for you to experience discomfort while getting laser treatments. To help minimize pain, Rogers says that some of her clients take two Advils 30 minutes before their treatment.
When done correctly, waxing actually grabs onto the hair and pulls the follicle. This is why the area is smoother than after a shave, according to Rogers.
FACT: It is recommended that you allow hair to grow 1/8 of an inch before waxing.
“It’s surprising how many people think they need to shave before a wax,” says Rogers.”The longer the hair, within reason, the smoother of a wax you’ll receive.”
MYTH: Waxing grabs onto the skin in order to pull hair out.
When done correctly, waxing actually grabs onto the hair and pulls the follicle. This is why the area is smoother than after a shave, according to Rogers.
FACT: Hair grows back less quickly when waxing versus shaving.
Rogers attributes the slower growth to the hair follicle being completely removed during the wax process. “It is waiting for the next growth stage,” she adds.
MYTH: There is no need to exfoliate after waxing because the hair removal method does it for you.
Not entirely true. On the third day of post-waxing, Rogers recommends using a sugar scrub to exfoliate along with a natural form of salicylic acid like willow bark to keep the pores in the area closed and less prone to bacteria. Exfoliation also helps to minimize ingrown hairs.




.jpg?timestamp=1470846057382)


.png?timestamp=1470846714983)
